

Easy problems
Or, what a dental AI panel and a vaccine event reveal about how institutions avoid self-reflection

Welcome to The Third Hemisphere, where I try to make sense of how AI is reshaping work, thinking, and creativity, often by watching my own assumptions get upended.
In case you missed it: I published two new columns in The Transmitter this month. “Why expertise won’t protect you from AI’s influence,” which focuses on AI use and metacognition among experts, and “Is the scientific paper due to be replaced?,” on what happens next with scientific publishing when AI is overwhelming the system.
If you were forwarded this and want to subscribe, click below. If you want to support a real human writing about AI, upgrade to paid.
The easy problem
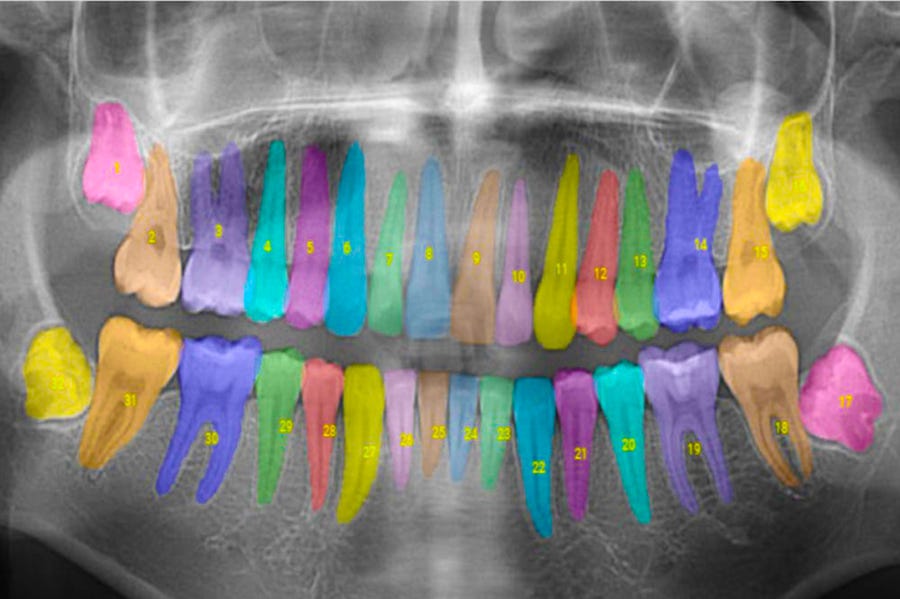
This week I found myself on a panel about, of all things, the role of AI in dentistry. The other folks on the panel were bigwig types: a dean of a dental school, president of a professional society, the CEO of a dental AI company whose software reads X-rays, and then there was me, who was enjoying being in a room with a dentist for the first time in my life.
During the hour-long conversation, whenever a thorny issue would come up — issues like: What happens when a young dentist trained on AI diagnostic tools can’t read an X-ray without one? What about the general-purpose chatbots that have no FDA clearance, no validation studies, no specific clinical guardrails, but that dentists are already using to look up questions, draft patient messages, and think through cases? — these institutional leaders would respond with a single phrase: critical assessment.
We need to train students to critically assess AI output. We need faculty to model critical assessment. We need rubrics and frameworks for critical assessment. I lost count somewhere around the fifth or sixth repetition, at which point “critical assessment” began sounding less like an actionable strategy and more like an incantation, something uttered to ward off uncomfortable questions.
On one hand, I get it: Critical assessment of AI output, or more broadly, guidelines on how to interact with AI responsibly, is important for professionals like doctors or dentists. But also, as I’ve argued before on the Third Hemisphere, AI guidelines are the easy problem. The hard problem is that people who understand AI guidelines perfectly still can’t follow them, even when they want to. The same person can vacillate between constructive and lazy AI use, sometimes within the same hour, because human cognition loves a good shortcut and general-purpose AI is engineered to make those shortcuts as enticing as possible. I’ve spent more than three years now coming up with AI best practices for graduate students and scientists, only to watch them struggle to consistently adhere to them. Yet, institutions keep hammering away at the need for…better guidelines.
The obsession with guidelines and critical assessment means that no one really engages with more challenging issues, like the incentive structures that determine whether a clinician defers to an AI diagnosis because they trust it or because they’re running fifteen minutes behind. Or the business models that will reward practices for seeing more patients per hour with AI scribes, regardless of whether anyone is critically assessing anything. When I raised system-level concerns, heads nodded. No one seems to disagree with the analysis, per se, but the fact that these concerns don’t tend to come up on their own, among deans and society presidents, the people who are best positioned to enact systemic reform, reveals how thoroughly the “critical assessment” frame has colonized the minds of the academic leadership caste.
Part of it, of course, is self-serving: framing AI usage as an individual problem puts responsibility where institutions want it. But I don’t think that’s the full story. Part is simply that “critical assessment” or “AI guidance” or whatever you want to call it is a solvable problem with a deliverable (a training module, a checklist, a workshop), looks good in a slide deck, and makes for a nice little perspective piece in an academic journal. Redesigning incentives is a messy political problem with no clean endpoint, but what I’d argue leadership is actually for. Sadly, I’m seeing institutions take the easy deliverable every time.
Vaccines and values at Pioneer Works

I recently subjected myself to a night of reliving the pandemic by attending an event at Pioneer Works in Red Hook for their Science & Society series on vaccines. David Wallace-Wells hosted Demetre Daskalakis (former CDC immunization director) and Jessica Malaty Rivera (epidemiologist, science communicator, person with an extremely good Instagram presence in a field not known for those). The event was billed as a conversation about trust, and in many ways it was a good one. Wallace-Wells asked probing questions. The crowd, while small for the venue, was engaged.
Daskalakis and Malaty Rivera were both passionate speakers and I believe they are motivated to improve public health. (I mean, I’m sure they are also motivated by citation metrics and attention and so forth but I don’t buy into narratives that public health academics are corrupt or nefarious in any deep way.) At the event, there was a lot of talk about the “politicization” of vaccines, framed as an external force: MAHA, anti-vax influencers, the reshaping of federal agencies by political appointees. The implicit stance, familiar from years of pandemic discourse, was that public health occupies neutral scientific ground and the challenge is defending that ground from political incursion.
I don’t think that’s quite right. And I say this as someone who shares, almost entirely, the values and goals of the people on that stage. Vaccines are among the most consequential inventions in human history. Childhood immunization rates should not be falling. Dismantling public health infrastructure is…bad.
But public health has never been neutral, and the pretense creates problems. As I wrote in Slate during the pandemic, no public health decision is purely scientific. When the CDC reduced the recommended isolation period during COVID from ten to five days and called it “motivated by science,” they were also weighing economic disruption, behavioral compliance, and the likelihood that a shorter window would get more people to isolate at all. Defensible trade-offs, sure, but trade-offs nonetheless. And weighing trade-offs requires making calls based on values. The health policy scholar Cecília Tomori put it well when I interviewed her: “Health policy decisions are always about values even if we don’t always articulate them. The values might be unstated versus explicit, but they are still there.”
What I saw at Pioneer Works was speakers who hold a set of values, things like mutual responsibility to each other, putting power in public institutions, achieving equity in health outcomes, and I watched those values underpin the entire discussion of evidence. But the discussion proceeded as though the evidence spoke for itself and happened to support exactly the outcomes they value. Any opposition is “politicized” or “misinformed.”
Consider a hypothetical parent in her early forties, college-educated, politically moderate-to-conservative. She vaccinated her kids on schedule because they were required to for school. She doesn’t have major reservations about the vaccines themselves. But she does have deep reservations about government-mandated vaccination schedules, that a public health agency should have the power to determine what goes into her children’s bodies or she has to home-school them. She values bodily autonomy. She’s skeptical of large institutions, public or private, making decisions on behalf of individuals.
From the vantage point of the Pioneer Works stage, this person is a victim of a misinformation problem. She might get lumped in with the conspiracy-minded. But her position isn’t a failure of scientific literacy. It’s a difference in values. She weighs individual autonomy more heavily than collective wellbeing. You can disagree with that weighting, I mostly do, but you can’t resolve the disagreement by showing her more data on vaccine efficacy, because vaccine efficacy is not the thing she is reacting to.
Of course, in the real world, this hypothetical parent may not quite exist, because the fractured media system of today means value systems and wrong facts get all tangled up together. I’d guess that many people with value systems that make them prone to vaccine hesitancy also are more likely to hold incorrect beliefs about basic facts — about ingredients or side effects, for example — because of their media diet. I’m not denying that misinformation is real and that it causes harm. But the public health establishment puts a lot of effort into the wrong-facts dimension, which is a sort of easy problem itself. In so doing, they obscure that choosing which evidence to foreground, which risks to emphasize, which trade-offs to accept are acts of judgment shaped by values. Pretending otherwise feels if not quite dishonest, then at least unexamined. It’s a classic case of Hume’s is-ought problem and why the liberal mantra to “follow the science“ is literal nonsense: It’s conceptually flawed to arrive at prescriptive statements solely from factual statements.
I don’t have a clear set of recommendations here (this is something I want to write about at more length, and I suspect the real essay is longer than a newsletter subsection). But I’ll say this much: CDC trust went from over 80 percent in 2019 to 44 percent by January 2022. Some of that is over-politicization, misinformation, and bad-faith actors who play fast and loose with the evidence. But some of it is people correctly sensing that values were shaping recommendations while health agencies pretend they are just “presenting the science.” Public health might be better served by owning its values explicitly and arguing on those grounds, rather than insisting on a neutrality that much of the public has, in any case, stopped believing in.
Risk assessment is not an exact science. One size does not fit all. There have certainly been bad vaccines pulled from the market. And people die every year from flu vaccine reactions. Pulling money from studies and testing is not the way to address the problem. Having known folks who survived polio I was glad of the vaccine when I was a child. I have friends that have brought their kids up without vaccines. But they use homeopathy, diet, etc to keep their immune systems strong. Some kids just do not have strong immune systems. Just keep them home when they are sick. And masks do help if you have ever travelled in many asian countries and seen them in use long before covid. Good article, makes one think.
Very well done. Highly recommended.